
My field was Population Studies -- basically the demography of who gets sick and why, often with an emphasis on "SES" or socioeconomic status. That is, the effect of education, income and occupation on health and disease. My Master's thesis was on socioeconomic differentials in infant mortality, and my dissertation was a piece of a large study of the causes of death in the whole population of Laredo, Texas over 150 years, with a focus on cancers. Death rates in the US, and the industrialized world in general were decreasing, even if ethnic and economic differentials in mortality persisted.
So, I was especially interested in the latest episode of the BBC Radio 4 program The Inquiry, "What's killing white American women?" Used to increasing life expectancy in all segments of the population for decades, when researchers noted that mortality rates were actually rising among lower educated, middle-aged American women, they paid close attention.
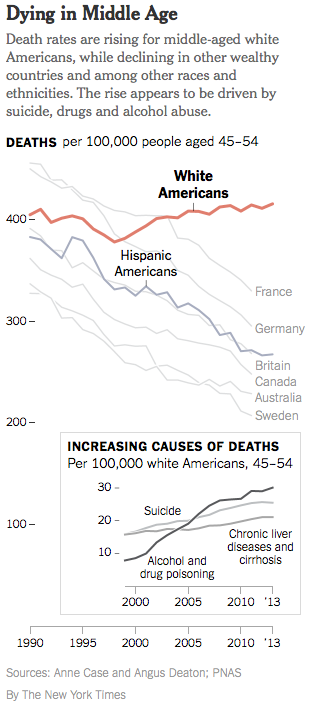
A study published in PNAS in the fall of 2015 by two economists was the first to note that mortality in this segment of the population, among men and women, was rising enough to affect morality rates among middle-aged white Americans in general. Mortality among African American non-Hispanics and Hispanics continued to fall. If death rates had remained at 1998 rates or continued to decline among white Americans who hadn't more than a high school education in this age group, half a million deaths would have been avoided, which is more, says the study, than died in the AIDS epidemic through the middle of 2015.
What's going on? The authors write, "Concurrent declines in self-reported health, mental health, and ability to work, increased reports of pain, and deteriorating measures of liver function all point to increasing midlife distress." But how does this lead to death? The most significant causes of mortality are "drug and alcohol poisonings, suicide, and chronic liver diseases and cirrhosis." Causes associated with pain and distress.
 |
| Source: The New York Times |
The Inquiry radio program examines in more detail why this group of Americans, and women in particularly, are suffering disproportionately. Women, they say, have been turning to riskier behaviors, drinking, drug addiction and smoking, at a higher rate than men. And, half of the increase in mortality is due to drugs, including prescription drugs, opioids in particular. Here they zero in on the history of opiod use during the last 10 years, a history that shows in stark relief that the effect of economic pressures on health and disease aren't due only to the income or occupation of the target or study population.
Opioids, prescribed as painkillers for the relief of moderate to severe pain, have been in clinical use since the early 1900's. Until the late 1990's they were used only very briefly after major surgery or for patients with terminal illnesses, because the risk of addiction or overdose was considered too great for others. In the 1990's, however, Purdue Pharma, the maker of the pain killer Oxycontin, began to lobby heavily for expanded use. They convinced the powers-that-be that chronic pain was a widespread and serious enough problem that opioids should and could be safely used by far more patients than traditionally accepted. (See this story for a description of how advertising and clever salesmanship pushed Oxycontin onto center stage.)
Purdue lobbying lead to pain being classified as a 'vital sign', which is why any time you go into your doctor's office now you're asked whether you're suffering any pain. Hospital funding became partially dependent on screening for and reducing pain scores in their patients.
Ten to twelve million Americans now take opioids chronically for pain. Between 1999 and 2014, 250,000 Americans died of opioid overdose. According to The Inquiry, that's more than the number killed in motor vehicle accident or by guns. And it goes a long way toward explaining rising mortality rates among working-class middle-aged Americans. And note that the rising mortality rate has nothing to do with genes. It's basically the unforeseen consequences of greed.
Opioids are money-makers themselves, of course (see this Forbes story about the family behind Purdue Pharma, headlined "The OxyContin Clan: The $14 Billion Newcomer to Forbes 2015 List of Richest U.S. Families;" the drug has earned Purdue $35 billion since 1995) but pharmaceutical companies also make money selling drugs to treat the side effects of opioids; nausea, vomiting, drowsiness, constipation, and more. Purdue just lost its fight against allowing generic versions of Oxycontin on the market, which means both that cheaper versions of the drug will be available, and that other pharmaceutical companies will have a vested interest in expanding its use. Indeed, Purdue just won approval for use of the drug in 11-17 year olds.
In a rather perverse way, race plays a role in this epidemic, too, in this case a (statistically) protective one even though it has its roots in racial stereotyping. Many physicians are less willing to prescribe opioids for African American or Hispanic patients because they fear the patient will become addicted, or that he or she will sell the drugs on the street.
"Social epidemiology" is a fairly new branch of the field, and it's based on the idea that there are social determinants of health beyond the usual individual-level measures of income, education and occupation. Beyond socioeconomic status, to determinants measurable on the population-level instead; location, availability of healthy foods, medical care, child care, jobs, pollution levels, levels of neighborhood violence, and much more.
Obviously the opioid story reminds us that profit motive is another factor that needs to be added to the causal mix. Big Tobacco already taught us that profit can readily trump public health, and it's true of Big Pharma and opioids as well. Having insinuated themselves into hospitals, clinics and doctors' offices, Big Pharma may have relieved a lot of pain, but at great cost to public health.
2 comments:
The rise in mortality rate in males has been shown to be due in part to a statistical error, i.e. the lack of age-standardization. Andrew Gelman has discovered and written about this (see e.g. here: http://www.stat.columbia.edu/~gelman/research/unpublished/age_adj_letter_4.pdf):
»The mortality rate among white non-Hispanic American women increased from 1999–2013. Among the corresponding group of men, however, the mortality rate increase from 1999–2005 is nearly reversed during 2005–2013.«
Thanks. There's an argument to be made that the economic downturn was harder on women than men, especially in rural areas. This is consistent with the data, though may or may not be the explanation.
Post a Comment